

Covid-19: What Can The Data Tell Us?

I present here selected data from a very lengthy analysis: Evidence over hysteria — COVID-19 . I got the link from Powerline, but my selection of data is substantially different. If you follow the link and read the entire presentation, you'll see that the author is very much of the view that what's currently going on is an unwarranted panic. At the end he urges readers:
Don’t let them forget it and vote
These days are precarious as Governors float the idea of martial law for not following “social distancing”, as well as they liked while they violate those same rules on national TV. Remember this tone is for a virus that has impacted 0.004% of our population. Imagine if this was a truly existential threat to our Republic.
The COVID-19 hysteria is pushing aside our protections as individual citizens and permanently harming our free, tolerant, open civil society. Data is data. Facts are facts. We should be focused on resolving COVID-19 with continued testing, measuring, and be vigilant about protecting those with underlying conditions and the elderly from exposure. We are blessed in one way, there is an election in November. Never forget what happened and vote.
Take that, Trumpkins!
I remain of the view that, based on what was and is known, Trump had no real alternative and ended up acting prudently.
Based on my reading of the data presented, a fair view is that--to anticipate my conclusion--Covid-19 is a very serious matter, but infection is far from an inevitability. Social distancing is warranted, but social isolation--to draw what I hope is a useful distinction--is probably not. That distinction may be useful going forward.
With that, we begin:
Against Panic
On a per-capita basis, we shouldn’t be panicking
...
Rank ordering based on the total number of cases shows that the US on a per-capita basis is significantly lower than the top six nations by case volume. On a 1 million citizen per-capita basis, the US moves to above mid-pack of all countries and rising, with similar case volume as Singapore (385 cases), Cyprus (75 cases), and United Kingdom(3,983 cases). This is data as of March 20th, 2020.
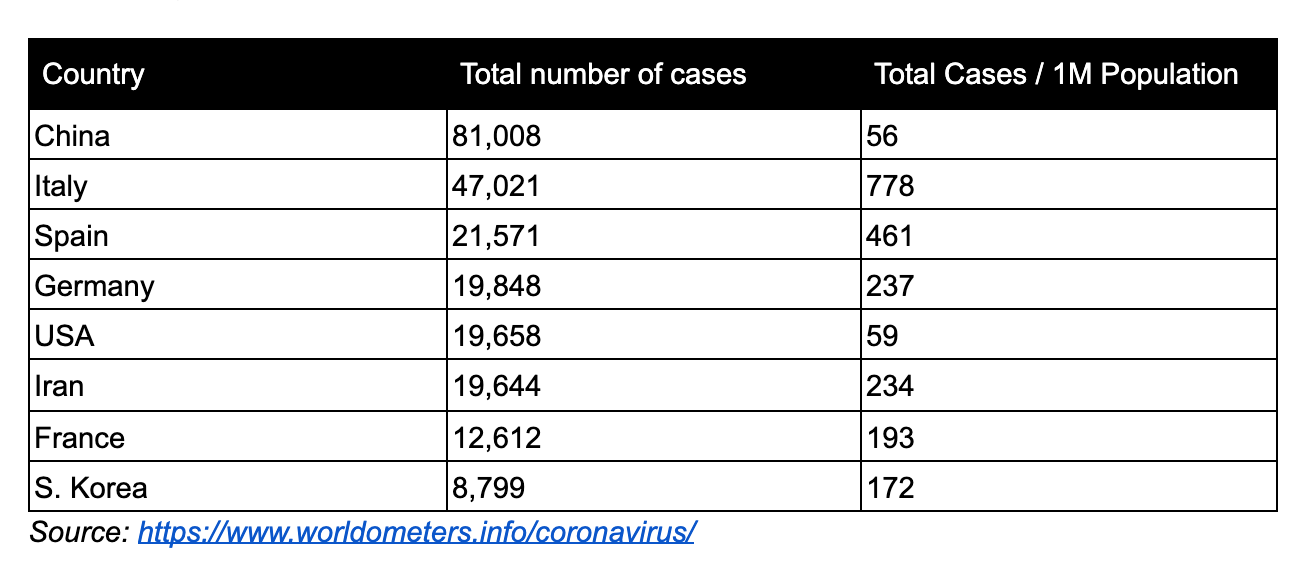
This suggests to me not simply that we're behind on testing--which we are, of course--but that the virus arrived here later than in other places. For reasons I can't explain. I say this simply from a seat of the pants view that if the virus had arrived here at the same time as in some other countries we'd have had a much larger number of serious cases presenting to hospitals than has been the case. That suggests that the US is taking strong measures at an earlier stage than other countries did, or that we may be on a par with Korea (based on other data).
The probability of catching COVID-19
The author calls this a "low" probability, but that's a relative term. It's better to compare it with the probability of catching seasonal flu. Seasonal flu is contracted by tens of millions of people every year. The number of people contracting Covid-19 would likely be some mix of "in addition to those contracting seasonal flu" and "people who contracted seasonal flu and are in a run down condition who then also contract Covid-19." Neither of those situations is a happy one if the rate of contraction of Covid-19 is similar to that of seasonal flu--which it is. Nevertheless, the numbers do also strongly suggest that avoidance is probably quite effective--and that perhaps we should be adopting higher measures of avoidance with regard to seasonal flu.
The World Health Organization (“WHO”) released a study on how China responded to COVID-19. Currently, this study is one of the most exhaustive pieces published on how the virus spreads.
The results of their research show that COVID-19 doesn’t spread as easily as we first thought or the media had us believe (remember people abandoned their dogs out of fear of getting infected). According to their report if you come in contact with someone who tests positive for COVID-19 you have a 1–5% chance of catching it as well. The variability is large because the infection is based on the type of contact and how long.
The majority of viral infections come from prolonged exposures in confined spaces with other infected individuals. Person-to-person and surface contact is by far the most common cause. From the WHO report, “When a cluster of several infected people occurred in China, it was most often (78–85%) caused by an infection within the family by droplets and other carriers of infection in close contact with an infected person.
From the CDC’s study on transmission in China and Princess Cruise outbreak -
A growing body of evidence indicates that COVID-19 transmission is facilitated in confined settings; for example, a large cluster (634 confirmed cases) of COVID-19 secondary infections occurred aboard a cruise ship in Japan, representing about one fifth of the persons aboard who were tested for the virus. This finding indicates the high transmissibility of COVID-19 in enclosed spaces.
Dr. Paul Auwaerter, the Clinical Director for the Division of Infectious Diseases at Johns Hopkins University School of Medicine echoes this finding,
“If you have a COVID-19 patient in your household, your risk of developing the infection is about 10%….If you were casually exposed to the virus in the workplace (e.g., you were not locked up in conference room for six hours with someone who was infected [like a hospital]), your chance of infection is about 0.5%”
According to Dr. Auwaerter, these transmission rates are very similar to the seasonal flu.
How is Covid-19 spreading in the real world? It's important to provide real world information rather than hypothetical scenarios.
Aerosolized Spread?
“This virus is not circulating in the community, even in the highest incidence areas across China,” WHO’s COVID-19 lead Maria Van Kerkhove said.
“Transmission by fine aerosols in the air over long distances is not one of the main causes of spread. Most of the 2,055 infected hospital workers were either infected at home or in the early phase of the outbreak in Wuhan when hospital safeguards were not raised yet,” she said.
True community spread involves transmission where people get infected in public spaces and there is no way to trace back the source of infection. WHO believes that is not what the Chinese data shows. If community spread was super common, it wouldn’t be possible to reduce the new cases through “social distancing”.
...
An author of a working paper from the Department of Ecology and Evolutionary Biology at Princeton University said, “The current scientific consensus is that most transmission via respiratory secretions happens in the form of large respiratory droplets … rather than small aerosols. Droplets, fortunately, are heavy enough that they don’t travel very far and instead fall from the air after traveling only a few feet.”
The media was put into a frenzy when the above authors released their study on COVID-19’s ability to survive in the air. The study did find the virus could survive in the air for a couple of hours; however, this study was designed as academic exercise rather than a real-world test. This study put COVID-19 into a spray bottle to “mist” it into the air. I don’t know anyone who coughs in mist form and it is unclear if the viral load was large enough to infect another individual As one doctor, who wants to remain anonymous, told me, “Corona doesn’t have wings”.
To summarize, China, Singapore, and South Korea’s containment efforts worked because community-based and airborne transmission aren’t common. The most common form of transmission is person-to-person or surface-based.
Surface Based Spread
COVID-19’s ability to live for a long period of time is limited on most surfaces and it is quite easy to kill with typical household cleaners, just like [seasonal] flu.
...
Presence doesn’t mean infectious. The viral concentration falls significantly over time. The virus showed a half-life of about 0.8 hours on copper, 3.46 hours on cardboard, 5.6 hours on steel and 6.8 hours on plastic.
According to Dylan Morris, one of the authors, “We do not know how much virus is actually needed to infect a human being with high probability, nor how easily the virus is transferred from the cardboard to one’s hand when touching a package”.
According to Dr. Auwaerter, “It’s thought that this virus can survive on surfaces such as hands, hard surfaces, and fabrics. Preliminary data indicates up to 72 hours on hard surfaces like steel and plastic, and up to 12 hours on fabric.”
Therefore, it's best to excercise caution when coming in contact with hard surfaces outside your home.
Geography and Climate
I don't believe we have data to support the author's contention that the change of seasons will mitigate Covid-19. It may, but it may not. It's presence in tropical areas like Singapore and Brazil or hot, dry summer areas (Australia) suggests that the mitigation would be temporary at best.
On the other hand, this now famous climate map illustrates that it does seem to spread most rapidly in a relatively narrow band (the green one). Unfortunately, it also illustrates that essentially all of Europe falls within that band, as do heavily populated areas of the US--New York, much of the Midwest, the Pacific Northwest:

How About Young People?
The data appears to show that those 19 and under are at a low risk for serious illness from Covid-19. However the data also negates, IMO, the authors belief that sending kids back to school is a good idea--young people are quite capable of spreading to those 20 and older:
According to the WHO’s COVID-19 mission in China, only 8.1% of cases were 20-somethings, 1.2% were teens, and 0.9% were 9 or younger. As of the study date February 20th, 78% of the cases reported were ages 30 to 69. The WHO hypothesizes this is for a biological reason and isn’t related to lifestyle or exposure.
...
However even if children and teens are not suffering severe symptoms themselves, they may “shed” large amounts of virus and may do so for many days, says James Campbell, a professor of pediatrics at the University of Maryland School of Medicine.
Children had a virus in their secretions for six to 22 days or an average of 12 days. “Shedding virus doesn’t always mean you’re able to transmit the virus”, he notes. It is still important to consider that prolonged shedding of high viral loads from children is still a risky combination within the home since the majority of transmission occurs within a home-like confined environment.
How Strong Is The "Viral Effect" Of Covid-19?
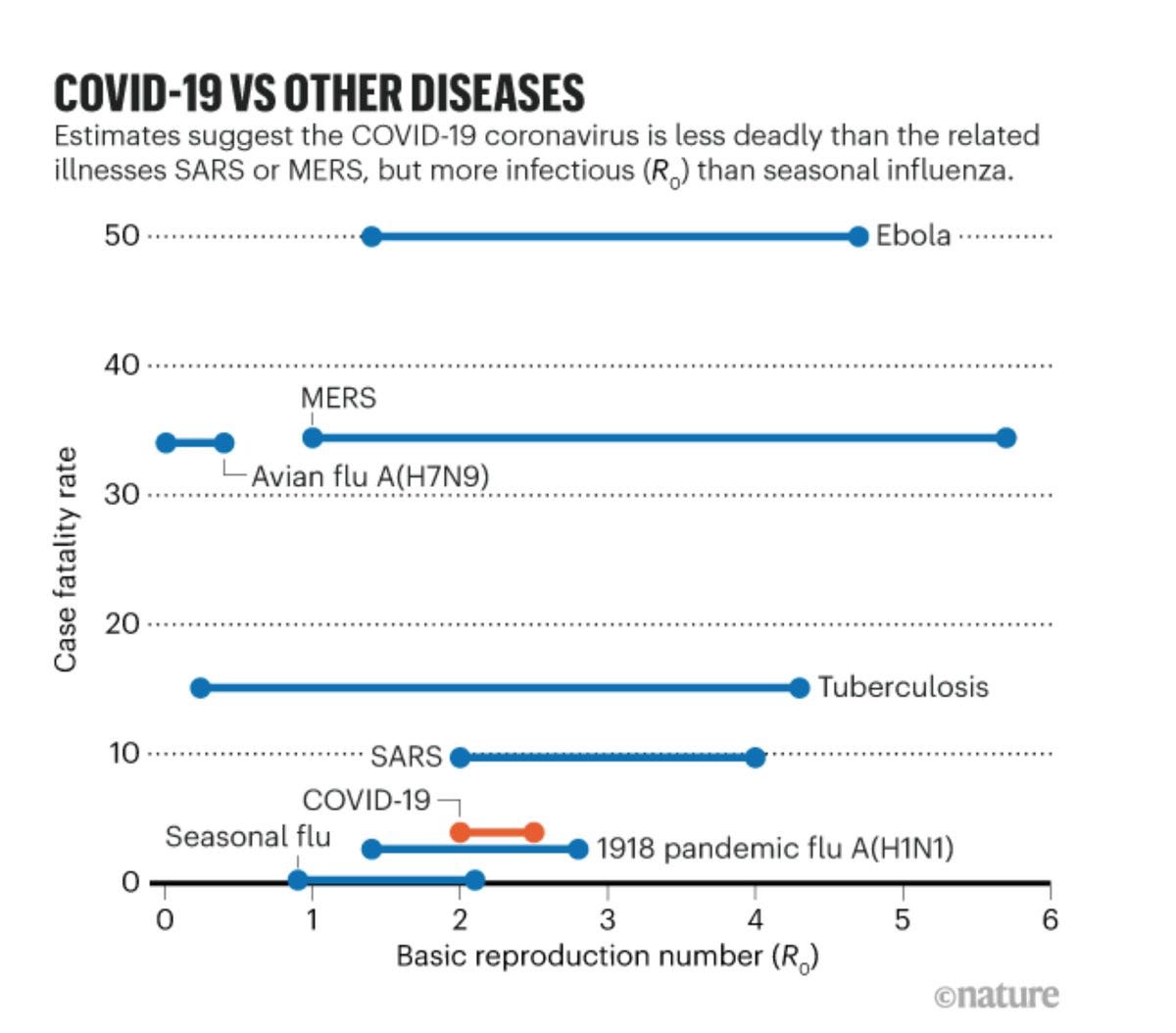
By "viral effect" we mean its ability to spread as measured by R-Nought. The short answer is, stronger than seasonal flu but less than other viruses:
While the true viral capacity is unknown at this moment, it is theorized that COVID-19 is more than the seasonal flu but less than other viruses. The average number of people to which a single infected person will transmit the virus, or Ro, range from as low as 1.5 to a high of 3.0
An Ro of 2.0 indicates that the virus could go exponential, so that's a real concern. Seasonal flu comes in around 1.3. Here's a nice graphic:
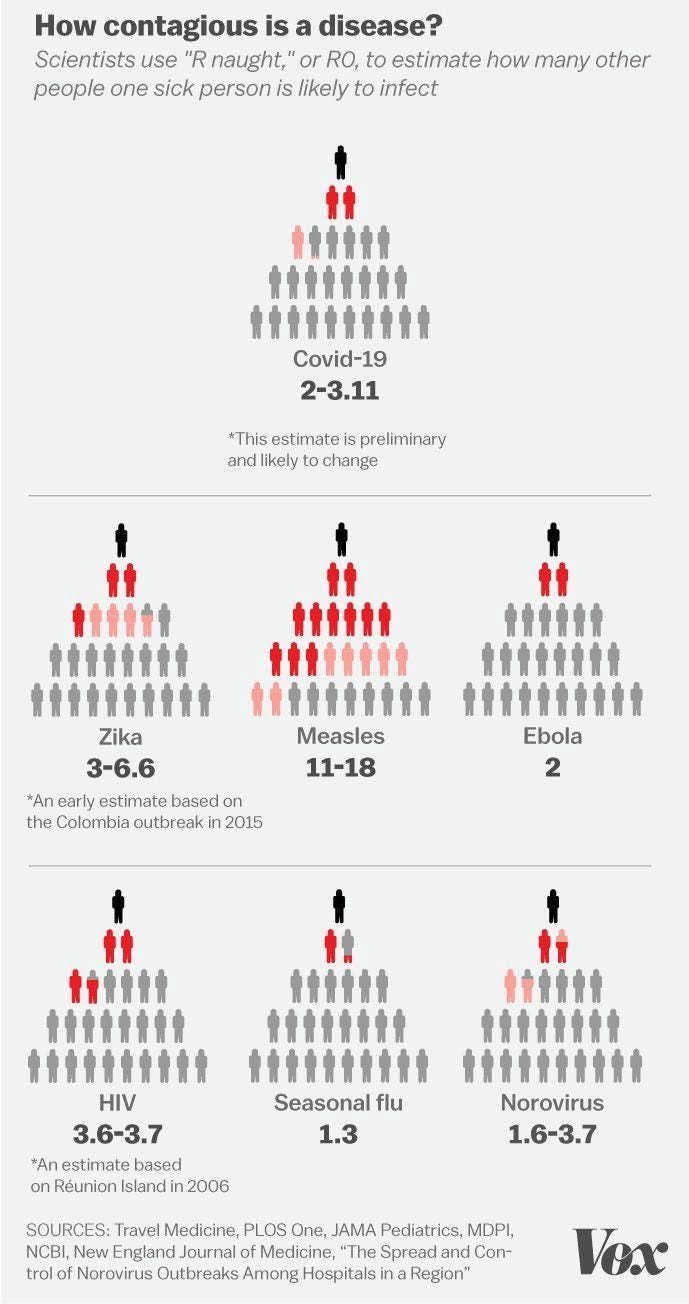
However, in the real world exponential growth always runs into logistic problems in maintaining that growth rate, so the growth rate tends to slow over time. Other concerns like the mortality rate then take over.
Asymptomatic Spread?
Probably vastly overrated:
“We still believe, looking at the data, that the force of infection here, the major driver, is people who are symptomatic, unwell, and transmitting to others along the human-to-human route,” Dr. Mike Ryan of WHO Emergencies Program.
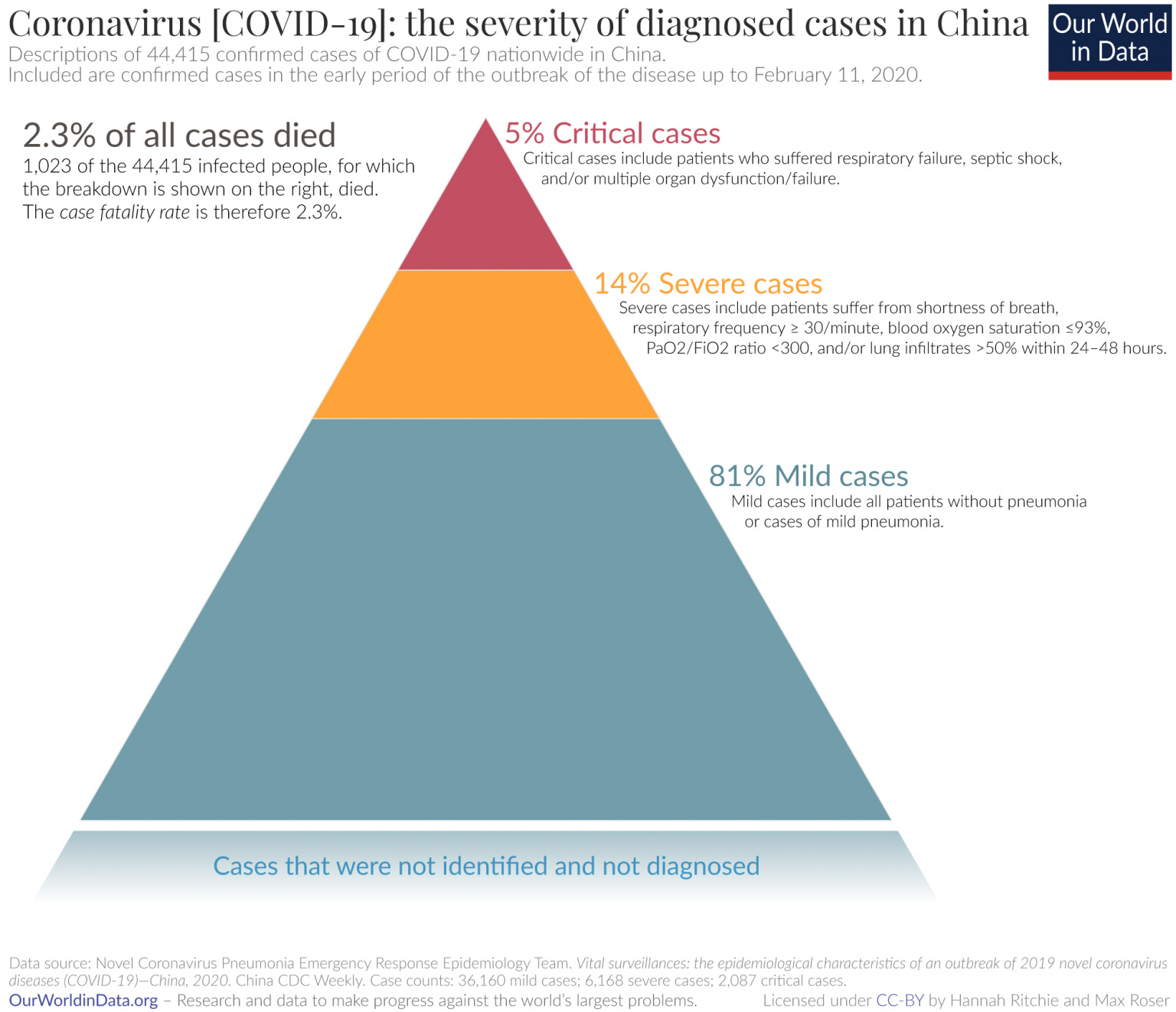
Rate Of Severe Illness?
Here's a nice graphic of the Chinese experience:
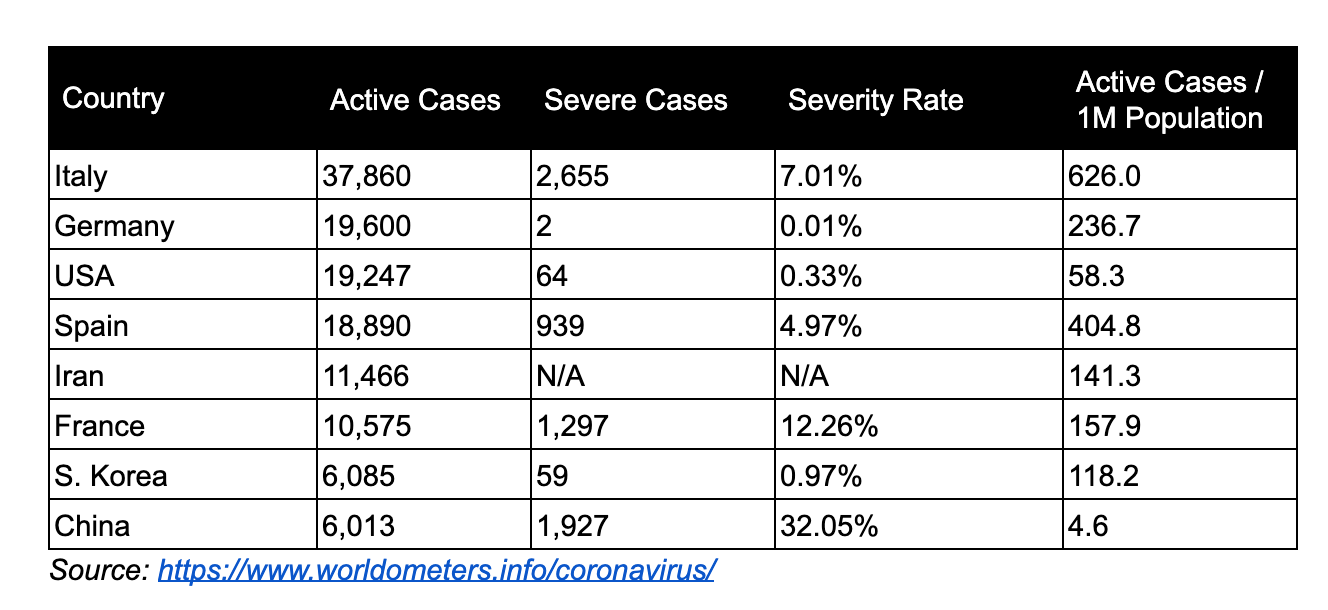
What will it be like in the US?
As of mid-March, the US has a significantly lower case severity rate than other countries. Our current severe caseload is similar to South Korea. This data has been spotty in the past; however, lower severity is reflected in the US COVID-19 fatality rates (addressed later).
Early reports from CDC, suggest that 12% of COVID-19 cases need some form of hospitalization, which is lower than the projected severity rate of 20%, with 80% being mild cases.
For context, this year’s flu season has led to at least 17 million medical visits and 370,000 hospitalizations (0.1%) out of 30–50 million infections. Recalling that only comparing aggregate total cases isn’t helpful, breaking down active cases on a per-capita basis paints a different picture on severity. This is data as of March 20th, 2020.
Two points here:
1. The flu season begins in September. Because flu does not spread as rapidly, doesn't achieve exponential growth rates, the case load is spread over many months. Note, too, that the hospitalization rate for all seasonal flu cases is much lower than that for Covid-19.
2. Thus we can see the importance of keeping overall Covid-19 numbers down--the overall case count. The reason for that is because if they grow rapidly in a shorter time period our hospital system will quickly be completely overwhelmed by the higher hospitalization rate.
Mortality Rates
This is where the rubber meets the road. The good news is that right now the US is more comparable to South Korea than to European countries. OTOH, South Korea famously took very aggressive steps, which suggests that the US did the right thing. Also, the US onset of infection appears to have lagged that of the rest of the world. Again suggesting that this is probably not the time to let up.
Since there is a wide range of opinion on what the mortality rate will end up being, I'll just offer some interesting charts and comparisons. Note two things:
1. Mortality is by no means confined to the over-70 gang, and
2. The mortality rate does appear to be more severe than that of seasonal flu.





The Bottom Line
The bottom line as I see it is that Covid-19 is a very serious matter, but that infection is far from an inevitability. Handwashing is good, but it seems to me that mask-wearing is probably vastly underrated as a preventive step--at least in the US. The reason is obvious--the US is very much unprepared and simply doesn't have anywhere close to the number of masks of any sort that it should have. The good news, however, is that homemade masks are, by all accounts (on the interwebs) quite effective. Given that the predominant means of infection is droplets rather than an aerosolized mist, the effectiveness of mask wearing in even more underrated than we already think.